

I’ve noticed many of my clients who complain of Achilles tendonitis and Haglund’s deformity have also expressed frustration in their healing process. Usually they voice dissatisfaction with their prescribed, boot’s effectiveness to relieve their foot pain, even after it’s been worn for a month, and then elaborate on additional pain that manifested in their hips and back since wearing the boot. I’ve also noted that in most cases orthotics were prescribed following the boot protocol, to immobilize the medial arch of the feet as a preventative measure.
While arch props may be helpful in their short-term use, their long-term use proves to be inadequate and a bit contradictory to the goal of healing and sustaining healthy foot function. You see, anything that abuts against the medial arch to prevent it from moving will throw foot mechanics off course and inhibit the arch’s ability to absorb the weight of the body. Instead, rigid props cause weight to rebound back into the bones of the transverse arch. This eventually weakens the ligaments that knit these four bones together, leading to further physical complications in other parts of the foot and body; including the recurrence of Achilles tendonitis.
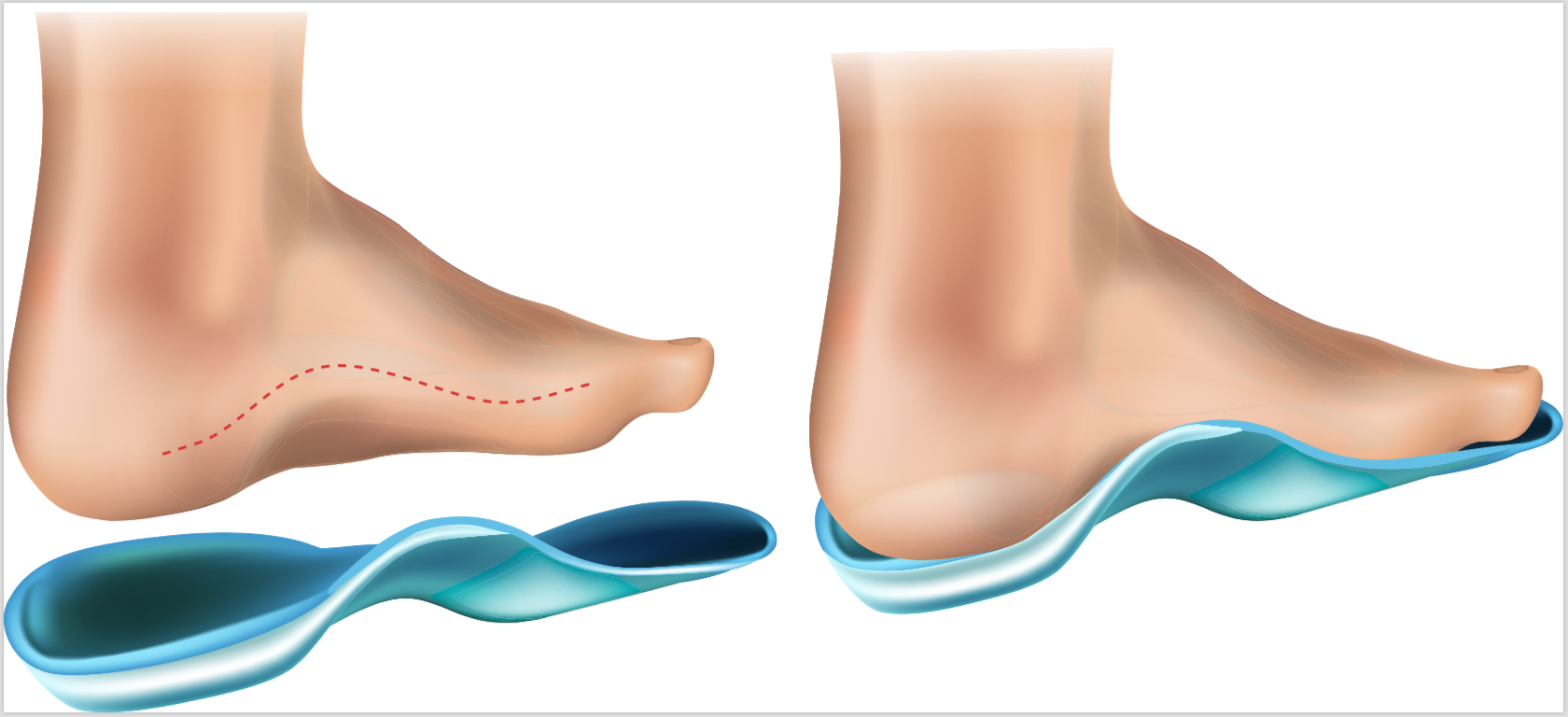
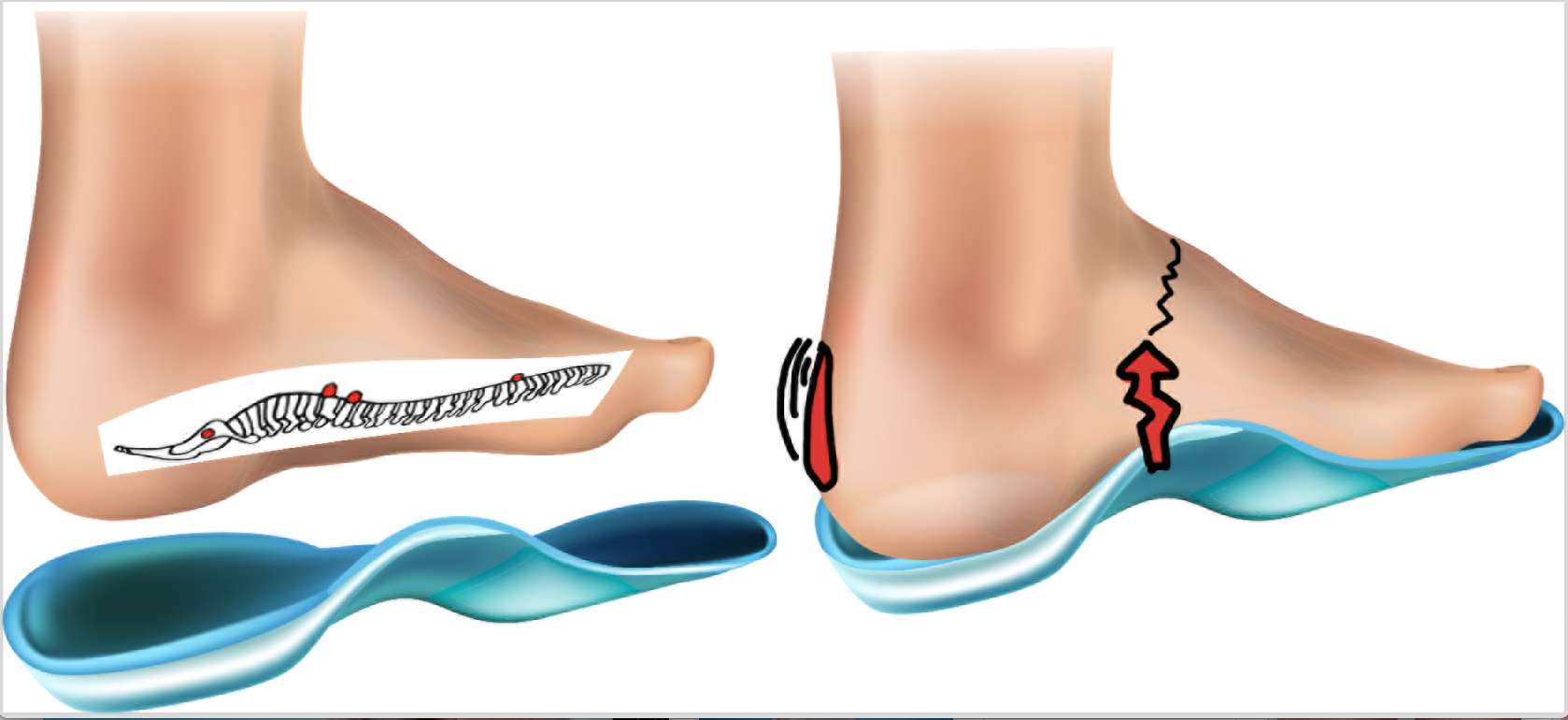
Long term use of rigid orthotics affect the vertebral spine and bones of foot.
Without the benefit of spring and shock absorption provided by the foot’s medial arch, the force of weight against an unyielding arch support has also been known to rebound to the Achilles tendon causing it to tear from abrupt and misdirected weight. The propelling function of the gastrocnemius and soleus muscles become interrupted, and subsequently, repetitive, brunt force inflames their tendon attachment on the posterior heel. This condition is called Achilles Tendonitis, which in its worse state of inflammation turns into a condition known as Haglund’s deformity- aka pump-bump. Pump-bump, notoriously named for it’s occurrence with wearing pump-style shoes, is in essence, the onset of accessory tissue which develops and embeds within this large tendon to reinforce strength and preserve the tendon and bursa beneath from further threat. The more the site inflames, the larger the bump becomes.
Pump-bumps can also emerge on the back of the heels of runners from running up and down hills wearing rigid insoles in their shoes. Athletic shoe stores are popular for suggesting such shoes and employ trainers to watch their patrons’ foot mechanics with a keen eye for hyper-pronated feet. While I agreed this prop will raise a dismantled arch, it will also become a detriment to the feet and body, especially to the vertebrae of the spine which will then take the impact of rebounded weight between their discs and trigger bulging and premature degeneration. Running for exercise is bigger than ever, and therefore, in my opinion, the best case scenario is for athletic shoe stores to hire Structural Reflexology® foot assessors, to help runners achieve their highest potential, and then promote shoes that align with their philosophy. Structural Reflexologists use non-invasive tools to assess feet and weight bearing issues, and then, based on these findings, apply trademarked techniques to release muscle and joint tension on the foot and lower leg which allows broken down arches to find their normal position, balance, and strength. See tools to assess feet here.

Why are shoe inserts ineffective for long-term use?
While the use of inserts may be unavoidable in certain, severe cases, medial arch inserts, which are often built into shoes, disrupt the normal pathway of weight as the foot carries the body. In fact, their rigid design encourages weight to bypass an essential stage of movement meant to shift weight towards the transverse arch. This essential shift of weight initiates muscles which attach to the transverse arch to continue to direct weight along the foot to the toes in a descending manner from small to great toe. Long-term use of wearing rigid orthotics will eventually weaken toe function and their ability to keep balance for the upper body.
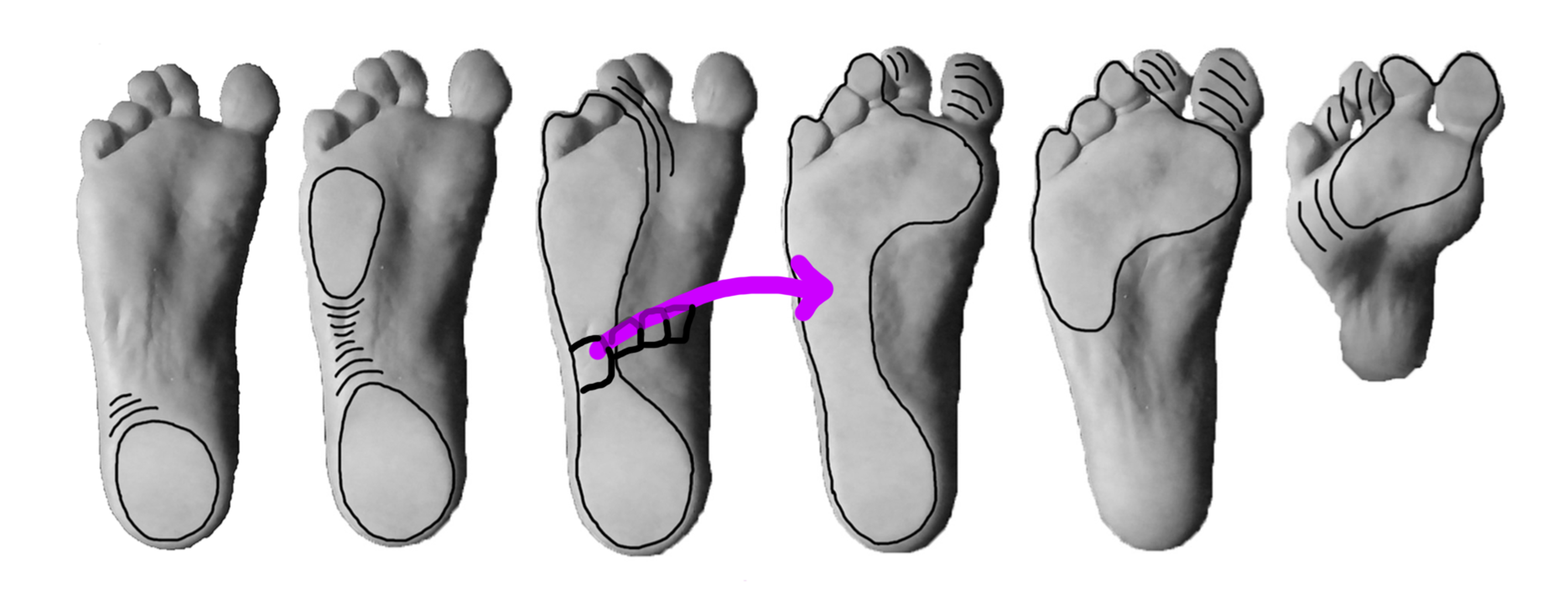
The normal, balanced foot goes through six stages of movement in one step. Weight received at the cuboid bone initiates muscles which attach to the transverse arch to direct weight along the foot to the toes.
To recap this stage of foot problem, Achilles tendonitis issues often happen when the medial arch is inhibited in its ability to spring and shock absorb, and it subsequently loses its recoil. Furthermore, when rigid orthotics prevents the medial arch from moving, the lateral (weight bearing) column of the foot takes too much responsibility for the load and this disorganizes the natural flow of how muscles move the foot and carry the body.
What you can do about it!
- REST is the best treatment for inflamed Achilles tendons. Ice will keep inflammation under control. Dunk your feet in a bucket of ice water for 1-5 minutes (depending on your tolerance) then let your foot warm up naturally, then re-dunk. Repeat x 3.
2. STRUCTURAL REFLEXOLOGY® will help to calm the nervous system while also releasing muscle and ligament tension areas on the foot and lower leg. Learn Here

3. PROPRIOCEPTIVE NEUROMUSCULAR FACILITATION (PNF) stretching. While the client lies comfortably in a prone position, bend their knee about 30-45 degrees and place the plantar side of their foot against your hip. To be most effective, their foot must be flush against your hip as opposed to just the toes contacting your hip. GENTLY, use pads of thumbs and fingers alternately to glide down the posterior leg from the heel toward the knee, being careful to avoid the popliteal fossa (hollow area in the back of the knee) . PNF stretching helps release muscle fibers that have become adhesive which likely developed from lack of spring in the medial arch. Keep the foot in this position the entire time for the greatest stretch. PNF takes 2-5 minutes on each leg to begin with. We do not want to overdo to avoid secondary inflammation. Apply a soft ice pack, or bag of frozen peas on the affected area immediately after PNF for about 5-10 minutes.
4. WALKING for 10-15 minutes (especially barefoot on grass), after receiving reflexology and PNF stretching will help lymph to penetrate, cleanse, and heal the affected area and also help reduce inflammation.
5. SLOWLY, LOWER HEELS on a stair, hold for 3 seconds, then slowly raise heels and hold for 1 second, repeat 10 times, morning and evening. Best results happen when inflammation is not acute.
*Before sending your client on a walk be sure the shoes they wear fit properly. Find tips to keep feet healthy and learn to measure feet in length from toe-to-heel, and the medial arch which runs from the MPJ to the heel, here.
One Response to 5 ways to relieve Achilles tendonitis and Haglund’s deformity.